Healthcare worker inspecting antibiotic medicines to identify counterfeit products in Africa. Freepik
Every year, more people in Africa die from drug-resistant infections than from HIV, malaria, or tuberculosis. Africa already carries the heaviest burden of infectious disease in the world, yet the medicines meant to fight those infections are losing their power, and the existence of counterfeit antibiotics is a major reason infections are spreading even with treatment (1).
In 2019, bacterial Antimicrobial Resistance (AMR) (the ability of bacteria to survive and grow despite antibiotic treatment) was linked to an estimated 1.05 million deaths across the African region under the World Health Organisation (WHO) (1). Of those 1.05 million deaths, 250,000 were directly caused by AMR, not by the infection itself, but by the fact that the drugs no longer worked (1). A 2024 study projected that by 2050, 4.1 million of the 10 million expected worldwide AMR deaths will occur in Africa (2).
These high death numbers reflect an urgent need to trace and tackle AMR, including what causes it, and what sustains it. Research findings have identified counterfeit antibiotics as one of the major factors that fuel AMR in Africa. Read on to learn how this happens.
What Are Counterfeit Antibiotics?
Counterfeit antibiotics is a broad term used to describe both substandard and falsified antibiotics.
- Substandard antibiotics: These are antibiotics made from genuine products, but do not meet the required quality standard. It may be that they do not have enough ingredients, were poorly manufactured, or were stored in unsafe conditions, such as heat or humidity. The label is real, the problem, however, is what is inside the antibiotics, what is missing, or how it has been kept (3).
- Falsified antibiotics: These are antibiotics that are deliberately produced to deceive. They are designed to look like a legitimate medicine, but they contain the wrong ingredient, an insufficient dose, or no active ingredient at all (3).
Both substandard and falsified antibiotics drive AMR and put patients’ lives at risk.
How Are They Different From Expired Medicines?
Expired antibiotics may be considered as a source of counterfeits, but they are quite different. An expired antibiotic may still retain some level of potency, but its effectiveness is unpredictable. Substandard and falsified antibiotics, however, may fail from the moment they are produced, regardless of the date printed on the packaging.
How Fake Antibiotics Directly Cause Antimicrobial Resistance
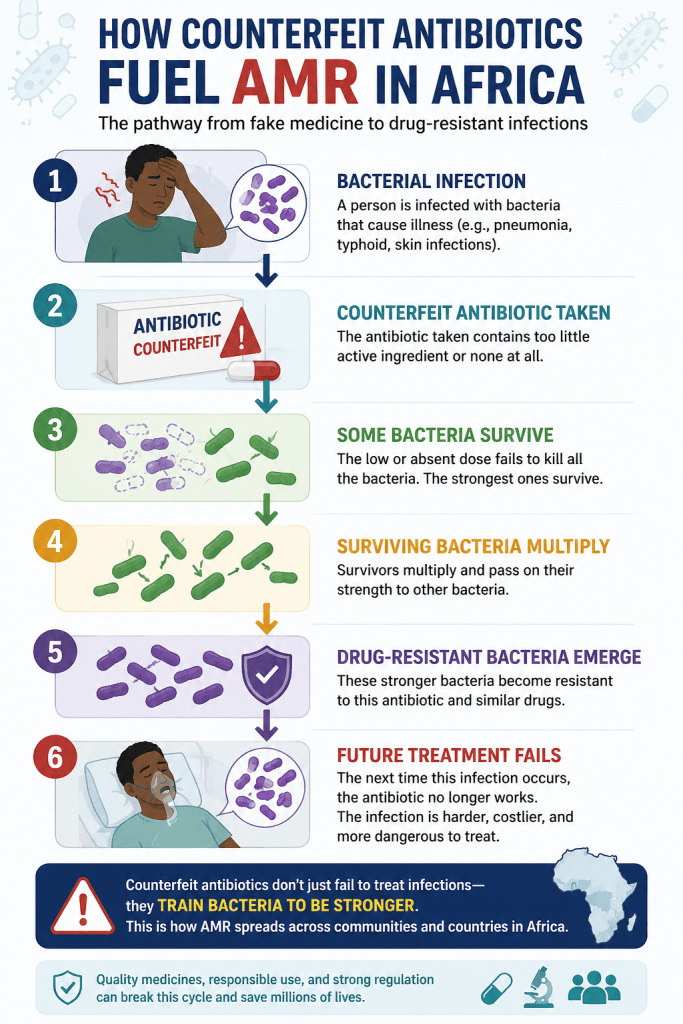
To understand the link between counterfeit antibiotics and AMR, it helps to first understand what antibiotics do. When taken at the correct dose, an antibiotic works by killing all or most of the bacteria causing an infection. For an antibiotic to work effectively, the dose must be sufficient, the timing must be consistent, and it should be taken in full, even if symptoms improve.
When a counterfeit antibiotic is taken instead of the original, it disrupts the mechanism that kills bacteria.
For instance, when a patient takes a tablet containing little or no active ingredient, as seen in counterfeits, the bacteria are exposed to the drug but not destroyed. As a result, some bacteria survive, and these survivors can withstand that antibiotic when they are exposed to it again. Over time, with repeated exposures, the bacteria can withstand antibiotics of a similar nature, regardless of dosage or duration – this is how Antimicrobial Resistance develops (4).
This process creates a condition called selective pressure, the mechanism by which the surviving bacteria multiply while weaker ones are eliminated (5). In this context, the antibiotic, rather than curing the infection, becomes a training exercise for the bacteria.
The result of selective pressure is a strain of bacteria that no longer responds to that drug. Treating the next patient with the same antibiotic will fail because the bacteria have already developed resistance, and so will treating the one after that. These resistant organisms can spread through direct contact, hospital environments, or community transmission, affecting even those without prior antibiotic exposure (5). This is how AMR, which started with a particular person, can affect people across different African countries.
How Big is the Counterfeit Antibiotics Problem in Africa
Studies across Africa consistently estimate that 22.6% of all medicines available in Africa are either substandard or falsified (6). Of all the medicine categories affected, antibiotics are the most common, accounting for 44.6% of all substandard and falsified medicines identified (6).
The number can even be higher, as some studies suggest that counterfeit drugs represent up to 50% of medicines in circulation in some parts of Africa (6).
This widespread circulation of counterfeit antibiotics is directly contributing to the AMR crisis Africa is currently suffering, as the continent records a rapid rise in drug-resistant infections across hospitals and communities alike.
The consequences of these variably high numbers of counterfeit antibiotics go beyond AMR to loss of life. According to research findings published in Frontiers in Pharmacology, approximately 169,000 children die from pneumonia each year in Africa as a direct result of substandard medicines (7). Another group of about 158,000 die from malaria for the same reason (7). These are children who received recommended treatment, but the medicine simply did not work because the disease-causing organism is stronger than the medicine that should kill it.
Which African Countries Are Most Affected?
The use of counterfeit antibiotics in Africa is widespread, but some regions and countries are affected more than others.
Across the continent, the overall prevalence of these poor-quality medicines is estimated to range from 18.7% to 22.6% of available treatments, with antibiotics making up the majority at 44.6% of those fake or substandard supplies (6). The high use of antibiotics in these parts of Africa leads to high cases of AMR, as inappropriate drug use and widespread exposure to counterfeit antimicrobials drive resistance upward (6).
As a result, the impact varies drastically by country; for example, Ghana has seen some of the highest rates, with one study revealing that 66.4% of sampled antibiotics were substandard (6). In East Africa, Kenya has documented a 37.7% prevalence rate for substandard amoxicillin, while falsified amoxicillin has also been reported in Central and West African nations like Cameroon and the Central African Republic (6).
Conversely, southern nations show a different trend as no counterfeit medicines were identified in South Africa in a major 2018 study, and only a limited number have been seen in Botswana and Namibia due to their stricter supply controls and dedicated enforcement units (6).
The continued circulation of counterfeit antibiotics in Africa is sustained by several factors, ranging from weak regulatory enforcement to supply chain structures and distribution. For instance, most countries in Sub-Saharan Africa (SSA) depend heavily on imported Active Pharmaceutical Ingredients (APIs). Because of this, when the imports travel through poorly regulated distribution networks, the risk of deliberate tampering and degradation multiplies at each stage (8).
Beyond API imports, the final distribution channels, specifically the private sector, which includes informal drug vendors, unlicensed pharmacies, and open medicine markets, are particularly vulnerable and highly fragmented across most countries in SSA. This creates solid gaps that counterfeit manufacturers and traders actively exploit (8).
The problem of AMR, partly created by counterfeit antibiotics in Africa, has received limited intervention, as only 5 out of the 46 countries in the WHO African region regularly monitor national antimicrobial consumption. Of the same 46 countries, just 16 use antibiotic consumption data to inform policy changes (8). Without this data, it is nearly impossible to track resistance trends or the quality of the medicines being dispensed.
Related: Why Maternal Mortality Remains High in Africa
Who Pays the Highest Price of Antimicrobial Resistance
AMR creates numerous harms and consequences that affect various individuals and age groups differently.
The most affected group is children, particularly those treated for pneumonia and malaria with falsified medicines that never had a chance of working (7). Communities in rural or remote areas face increased disadvantage because they live farther from verified pharmacies, formal health facilities, and regulatory bodies that oversee the distribution of quality medicines. As a result, they are most likely to encounter poor-quality medicines sold through informal markets.
People living with HIV, tuberculosis, or other chronic infections are another group that faces the harmful risks of AMR. Incomplete treatment caused by counterfeit antibiotics accelerates resistance in infections that are already difficult to manage. For these patients, a drug-resistant infection is often a death sentence, because second-line and third-line treatment options are scarce and expensive across different African countries.
Healthcare workers, too, are caught in the treatment failures AMR creates. The doctors prescribe correctly, the nurses administer accurately and manage adequately, yet patients return unwell because the medicine they dispensed contained almost nothing of what was promised on the label. This creates an overwhelming workload for them and even a likelihood of disease outbreak. It can also cause patients to lose trust in them and, as a result, seek alternative treatments that can potentially be dangerous.
Related: The Tuberculosis Detection Gap in Africa
What Is Being Done to Manage the Problem

To protect the public from dangerous fake antibiotics, several major initiatives are actively working across Africa to clean up the medicine supply chain. They include the following:
1. Unified Continental Oversight
The WHO has newly united with the African Medicines Agency (AMA) to coordinate drug regulations across different African countries. It harmonizes safety reviews so fake medicines cannot easily cross porous borders.
2. Immediate Testing and Mobile Verification
Pharmacies are increasingly adopting instant digital tools to check drug safety. Small-scale programs also now allow consumers to scratch a label on an antibiotic box to test a code and verify its authenticity instantly. Meanwhile, customs border officers can use handheld scanning devices to test the chemical makeup of pills on the spot.
3. Tightening Local Drug Distribution
Countries are replacing chaotic open-air drug markets with centralized, government-monitored wholesale centers. At the same time, national enforcement agencies are tightening prescription laws so antibiotics are only given out by licensed pharmacies.
4. Global Warning Systems
This is a WHO global surveillance network that allows African nations to share information rapidly. If a toxic or fake batch of antibiotics is discovered in one country, an immediate alert is blasted to neighboring countries to seize the bad batches before they are sold.
Despite the solutions on the ground, the gaps currently remain wide as only less than 1/8th of countries in the WHO African region regularly monitor national antimicrobial consumption (8). Regulatory enforcement of pharmaceutical quality also remains inconsistent across most African markets, and local pharmaceutical manufacturing capacity remains concentrated in just four countries (Nigeria, South Africa, Kenya, and Ghana), leaving the majority of the continent entirely dependent on imports (8).
Related: END TUBERCULOSIS BY 2030: A DOABLE COURSE OR POLICY RHETORIC IN RURAL COMMUNITIES?
What Needs to Change
Addressing counterfeit antibiotics as a driver of AMR demands action at every level of the supply chain, from the manufacturer to the patient’s hand.
First, pharmaceutical regulation must be strengthened and enforced consistently. Medicines entering African markets must undergo robust quality testing, particularly at ports of entry. WHO prequalification, a rigorous certification process for medicine quality, should be expanded to support more African manufacturers in producing locally at scale.
Second, public education should be widely enforced. Patients who understand why they should purchase medicines only from authorised sources, and why completing a full antibiotic course is essential, become part of the solution. Health literacy in every context is not a luxury, but a clinical tool that can combat most public health concerns, especially AMR.
Third, pharmaceutical manufacturers and distributors should be held to stronger ethical and regulatory accountability surrounding medicine production. The resistant bacteria spreading across Africa today did not emerge from nowhere. They were, in part, caused by counterfeit medicines sold as cures. Fixing that is not only a regulatory challenge, but a moral one.
Lastly, both healthcare workers and patients should be constantly prompted to adhere to hygiene practices. According to Gavi – the Vaccine Alliance, improving water, sanitation, and hygiene alone could prevent up to 20% of AMR-related deaths in Africa each year (1). This particular intervention does not require new technology, but sustained education and implementation of various infection prevention and control measures.
Conclusion
The power of antibiotics is slipping away across Africa, turning treatable infections like pneumonia and malaria into fatal conditions. While strengthening regulatory frameworks and deploying mobile verification tools are critical defensive steps, the ultimate solution also relies on public empowerment. Enhancing health literacy ensures that patients demand authentic drugs from licensed sources and complete their prescribed therapies. Combined with essential water, sanitation, and hygiene improvements, targeted community education can break the selective pressure driving AMR, preserving life-saving treatments for future generations.
References
- Joi P. Antimicrobial resistance emerges as a bigger killer in Africa than malaria, HIV or TB [Internet]. Geneva: Gavi, the Vaccine Alliance; 2024 Sep 17 [cited 2026 May 31]. Available from: https://www.gavi.org/vaccineswork/antimicrobial-resistance-emerges-bigger-killer-africa-malaria-hiv-or-tb
- Erasmus RT, Obi CL, Souda S. The scourge of antimicrobial resistance: Containing a global crisis. African Journal of Laboratory Medicine. 2024;13(1):1-3. Available from:
https://www.scielo.org.za/scielo.php?pid=S2225-20102024000100025&script=sci_arttext
- World Health Organization. Substandard and falsified medical products [Internet]. Geneva: World Health Organization; 2024 Dec 3 [cited 2026 May 31]. Available from:
https://www.who.int/news-room/fact-sheets/detail/substandard-and-falsified-medical-products
- Gulumbe BH, Adesola RO. Revisiting the blind spot of substandard and fake drugs as drivers of antimicrobial resistance in LMICs. Annals of Medicine and Surgery. 2023 Feb 1;85(2):122-3. Available from: https://journals.lww.com/annals-of-medicine-and-surgery/fulltext/2023/02000/revisiting_the_blind_spot_of_substandard_and_fake.9.aspx
- Nimmana BK, Nguyen AD. Antibiotic resistance. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2026 Jan- [updated 2026 Jan 31; cited 2026 May 31]. Available from:
https://www.ncbi.nlm.nih.gov/books/NBK513277
- Maluleke TM, Mekonnen BA, Ubaka CM, Paramadhas BD, Munzhedzi M, Kalungia AC, Hango E, Kumar S, Godman B, Meyer JC. Potential activities to reduce the extent of substandard and falsified antibiotics across Africa and associated antimicrobial resistance. Frontiers in Tropical Diseases. 2025 Sep 24;6:1634029. Available from:
https://www.frontiersin.org/journals/tropical-diseases/articles/10.3389/fitd.2025.1634029/full
- Chabalenge B, Sahota T, Ermolina I, Tanna S. Substandard and falsified medicines in Africa: healthcare systems challenges, supply chain issues, regulatory challenges and strategies to increase access to quality medicines. Frontiers in Pharmacology. 2025 Nov 18;16:1708784. Available from: https://www.frontiersin.org/journals/pharmacology/articles/10.3389/fphar.2025.1708784/full
- Olpengs D, Munjuri AK, Benson AE, Othman ZK, Adebisi YA. The supply chain lens of the burden of antimicrobial resistance in Sub-Saharan Africa. Discover Public Health. 2025 Dec 14;22(1):828. Available from:
https://link.springer.com/article/10.1186/s12982-025-01242-w