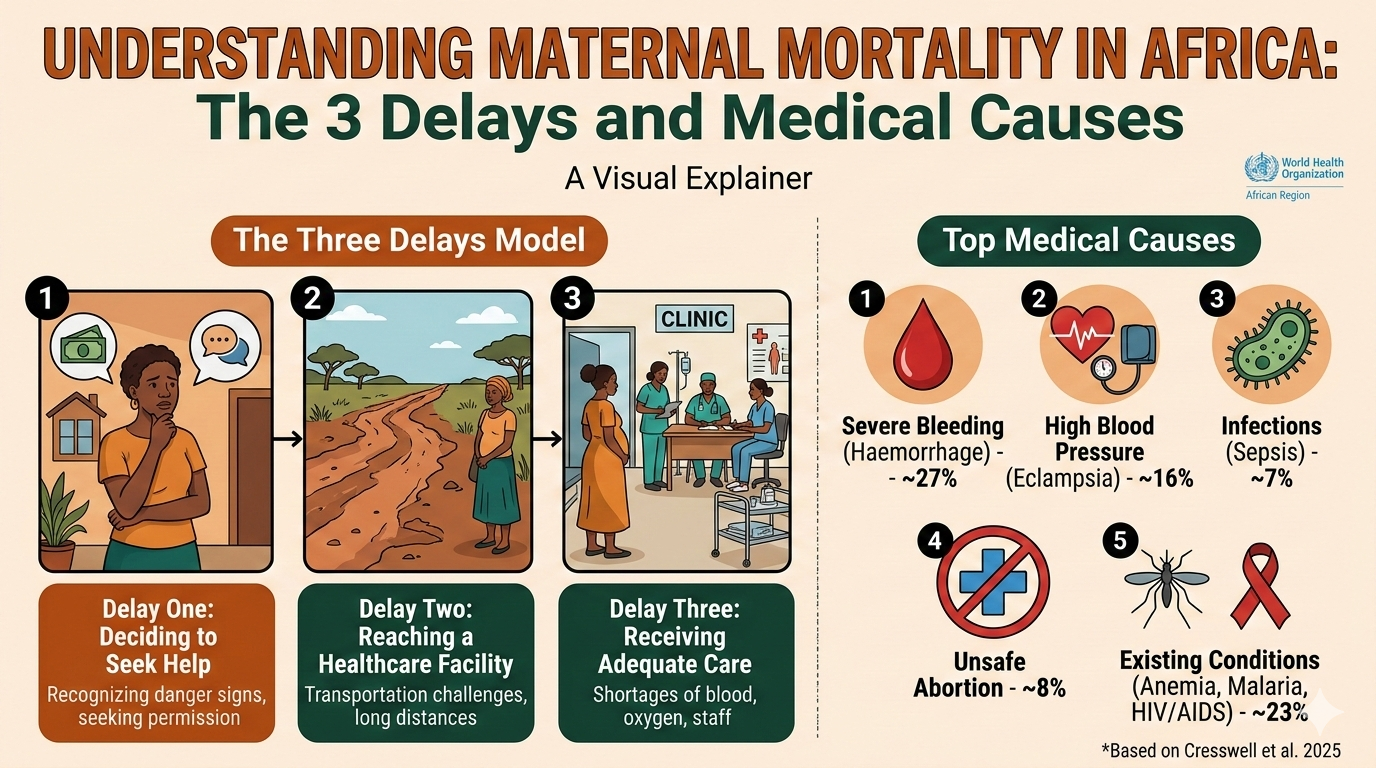
AI generated visual explainer on the causes of maternal mortality
Africa contributes 70% of all maternal deaths worldwide, with an estimated 487 women dying every day (1). Numerous factors, divided into two categories, contribute to these deaths from pregnancy and childbirth complications:
The first class is the “Three Delay Model,” which is a framework used to identify barriers to obtaining care during pregnancy or childbirth, specifically focusing on delays in decision-making, reaching a health facility, and receiving adequate care once there. These three delays are centred on a lack of knowledge, transport issues, and poor-quality services in health facilities.
The second class of factors that contribute to maternal deaths is the childbirth-associated medical conditions. This is a group of five health problems that can easily arise from pregnancy and labour processes, and when they interact with the three delays, they produce a high number of maternal deaths, as it is currently seen in Africa.
By examining these delays alongside the five primary medical causes of death, we can see exactly how the chain of care breaks down across the continent.
This article is a detailed supplement to our main explainer: Why Maternal Mortality Remains High in Africa.
The Three Delays of Maternal Mortality
Maternal deaths in Africa usually result from multiple medical failures. Instead, they happen because of a breakdown in a chain of events. Health experts use the “Three Delays Model” (Thaddeus & Maine, 1994) to show exactly where this chain breaks. The three-stage delay model explains that for a pregnant woman to survive, she must pass through three different stages without getting stuck. If she is delayed at any stage, her risk of dying increases.
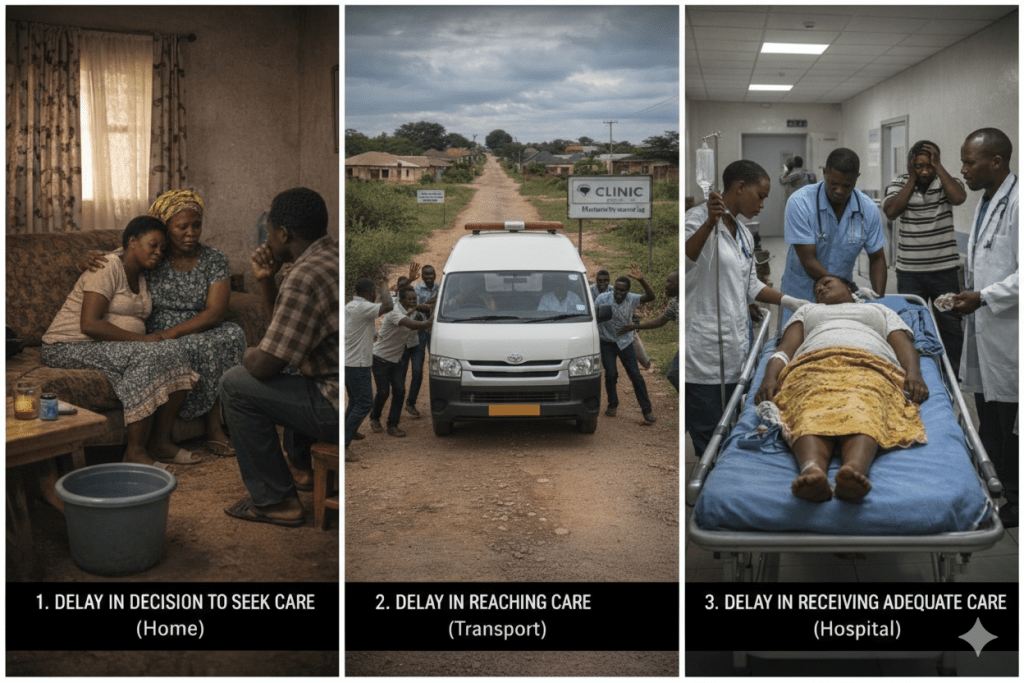
Delay One: Deciding to Seek Help
This is when a woman knows something is wrong, but she does not go to the hospital immediately.
In many African communities, this happens because women cannot make healthcare decisions by themselves. They need permission from their husband or mother-in-law. A study across 22 African countries found that the first delay (deciding to seek care) accounted for 26% of all maternal deaths (2).
However, in Ethiopia, this first delay was the biggest killer. It caused more deaths than any other delay (2). Pregnant women often delay seeking help because of the following reasons:
- They did not recognise the danger signs (they did not know bleeding or severe pain meant emergency)
- They thought the problem would go away by itself
- They had to get permission from family members first
- They were afraid of hospitals because of bad experiences before
- They believed traditional healers could help them better than health professionals
A 2024 study in the Wolaita Zone, southern Ethiopia, examined 410 mothers who gave birth in rural health centers between 2020 and 2022. The researchers found that 42.1% of mothers delayed seeking care when they went into labour (3). This means that nearly half of the women waited too long before deciding to go to the health facility.
The study identified the following as the causes of the delays:
- Unemployment: Unemployed mothers were 2.5 times more likely to delay seeking care compared to women who had jobs. This is mostly because they could not afford the transport money to the hospital.
- Illiteracy: Women whose husbands had no formal education were also more likely to delay. These husbands did not understand the importance of hospital deliveries, nor did they recognise danger signs.
- Poor health-seeking behaviour: mothers who had negative attitudes toward health facilities, like those who believed hospitals were unfriendly, uncomfortable, or unnecessary, were 1.7 times more likely to delay seeking care. Some women simply did not want to go to the hospital. They felt more comfortable at home, even when complications were developing.
By the time many of these women finally reached the health facility, their conditions had worsened, making it difficult for them to be saved, often due to the delays caused by their initial reluctance to seek help and the challenges they faced in transportation.
Delay Two: Reaching the healthcare facility
This is when a woman decides to seek help, but she cannot reach the hospital quickly. This second delay accounted for 15% of maternal deaths across Africa (2). But in some places, the numbers are higher.
A 2024 study carried out in Bale and East Bale zones of Ethiopia examined 407 mothers who had given birth in hospitals. The researchers found that 38.1% of pregnant women experienced high delays in reaching health facilities during pregnancy emergencies (4).
The study identified the following reasons as exactly why the delays happened.
- Distance: Distance was the biggest problem. Women who lived far from health facilities were 4.35 times more likely to arrive late at the hospital. When you live in a rural area with poor roads and no nearby hospital, even deciding quickly to seek help does not guarantee you will reach help in time.
- Poverty: Women with low monthly income were 1.87 times more likely to experience transport delays. This is because they could not afford to pay for transport immediately. When a woman is in labour, she needs to get to the hospital within hours. But if she has no money, she must first find someone to lend her transport fare.
The study revealed another harmful pattern. Women who had already delayed deciding to go to the hospital were 2.9 times more likely to also experience delays in actually reaching the hospital (4). This means that the delays compound. First, she waits too long to make the decision. Then, when she finally decides, she faces transportation problems. By the time she reaches the hospital, it may already be too late.
Other problems that cause the second delay include the following:
- Bad roads full of holes and mud
- No ambulances in rural areas
- No public transport at night
- Rivers with no bridges (some women have to wait for boats to cross rivers in certain regions)
Delay Three: Receiving Adequate Care at the Facility
The delay in receiving adequate care is the deadliest among the three delays. This is when a woman reaches the hospital, but the hospital cannot help her properly.
This third delay accounted for 61% of all maternal deaths in Africa (2). This means that deciding to seek help and getting to the hospital in time makes little difference if the hospital does not provide adequate, timely care.
The following factors contribute to the delay in receiving adequate care in healthcare facilities:
- Shortage of skilled health workers, like nurses and doctors
- Unavailability of essential resources like blood, oxygen, and certain medications.
- Unavailability of an operating theatre for emergency surgeries
- Absence of an ambulance to transfer patients to better hospitals
- Poor and irregular monitoring of patients, mostly due to understaffing
- Delayed referrals
The Medical Causes of Maternal Mortality
Now that you understand the three delays of maternal mortality, let’s discuss the medical conditions that lead to these deaths.
A 2025 study by Cresswell and his team on the causes of maternal deaths from 2009 to 2020 revealed the following as the main causes of maternal death:
1. Severe Bleeding (Haemorrhage)
This is the number one cause of maternal deaths. It contributes to about 27% of maternal mortality worldwide (5), with an even higher number in Africa.
Severe bleeding usually happens after childbirth, usually from the womb not contracting enough. Without quick medical help, a woman can bleed to death in a few hours.
The treatment is usually to give her an injection to stop bleeding or a blood transfusion if she has lost too much blood. But many African hospitals do not have these supplies; hence, the woman ends up dying.

2. High Blood Pressure (Hypertensive Disorders)
High blood pressure in pregnancy can be in the form of pre-eclampsia (very high blood pressure during pregnancy) or eclampsia (very high blood pressure plus seizures).
According to the 2025 study by Cresswell, hypertensive disorders cause about 16% of maternal deaths (5). Without proper care and management, a woman with eclampsia can die within hours.
The treatment for this very high blood pressure in pregnancy requires specific medications and close monitoring. However, many rural hospitals do not have these medications or trained staff, leading to the death of the woman.
3. Infections
About 7% of maternal deaths come from infections (5). Many African hospitals lack basic sanitation. Some delivery rooms do not even have running water; this increases the risk of infection.
Infections from childbirth can happen for a number of reasons, like:
- Delivery was done in unclean conditions
- Poor drainage of the afterbirth fluid
- Unsafe abortions
4. Unsafe Abortion
About 8% of maternal deaths come from complications from unsafe abortions.
In countries where abortion is illegal or restricted, like in Nigeria, women go to untrained people for abortions. These unsafe abortions cause severe bleeding, infections, and death.
5. Existing Medical Conditions (Indirect Causes)
About 23% of maternal deaths happen because the woman already had another disease (5). These diseases get worse during pregnancy and eventually lead to death.
Common conditions among pregnant women that contribute to maternal mortality include:
- Anaemia, also known as low blood level
- Malaria
- HIV/AIDS
- Heart disease
- Diabetes
A pregnant woman with severe anaemia is at a very high risk of dying during or after labour because her blood is already low. Therefore, if she bleeds, the blood available in her body will not be able to sustain her. And because many health facilities lack blood for transfusion, the woman has a very low chance of survival.
Conclusion
Every medical condition and logistical delay that kills mothers in Africa is preventable. We know the exact health problems, like severe bleeding and high blood pressure, that cause these tragedies. We also know how to manage them. However, medical knowledge alone is not enough if the chain of care is broken by delays in seeking, reaching, or receiving help.
While the three delays and medical conditions explain how these deaths happen, they do not explain the system failures that sustain these deaths.
To understand the systemic, socioeconomic, and political factors keeping these numbers high, and to see which African countries are successfully fighting to save women’s lives, return to our main guide: Why Maternal Mortality Remains High in Africa
References
1. World Health Organization. Regional Office for Africa. African region’s maternal and newborn mortality declining, but progress still slow [Internet]. Brazzaville: World Health Organization; 2025 Apr 7 [cited 2026 Feb 24]. Available from: https://www.afro.who.int/news/african-regions-maternal-and-newborn-mortality-declining-progress-still-slow
2. Muriithi FG, Ameh CA, Gakuo RW, Williams CR, Devall A, Coomarasamy A, Fawcus S. Variability in the Causes and Delay Factors Contributing to Maternal Mortality: Evidence From Maternal Death Surveillance Reports of 22 African Countries. BJOG: An International Journal of Obstetrics & Gynaecology. 2026 Jan;133(1):106-15. Available from:
https://obgyn.onlinelibrary.wiley.com/doi/full/10.1111/1471-0528.18342
3. Gelaw KA, Atalay YA, Zerefu F, Gebeyehu NA. Delays in the decision to seek care and associated factors among mothers who delivered in rural health centers in Wolaita Zone, Southern Ethiopia. Frontiers in Global Women’s Health. 2024 Jan 11;4:1236242. Available from:
https://www.frontiersin.org/journals/global-womens-health/articles/10.3389/fgwh.2023.1236242/full
4. Eshetu D, Aschalew Z, Bante A, Negesa B, Gomora D, Ejigu N, Geta G, Mersha A. Delay in reaching health facilities for emergency obstetric care and associated factors among postpartum mothers at Bale zones, Ethiopia. A cross-sectional study. PLOS Global Public Health. 2024 Feb 28;4(2):e0002964. Available from:
https://journals.plos.org/globalpublichealth/article?id=10.1371/journal.pgph.0002964
5. Cresswell JA, Alexander M, Chong MY, Link HM, Pejchinovska M, Gazeley U, Ahmed SM, Chou D, Moller AB, Simpson D, Alkema L. Global and regional causes of maternal deaths 2009–20: a WHO systematic analysis. The Lancet Global Health. 2025 Apr 1;13(4):e626-34. Available from:
https://www.thelancet.com/journals/langlo/article/PIIS2214-109X(24)00560-6/fulltext